|
FORUMS - Articles, questions, replies
Autoimmunity Research Foundation
Solving the enigma of 'autoimmunity' - one disease at a time
Benicar / Minocycline
Autoimmune' is the name given to the dozens of diseases characterized by the presence of Th1 inflammation. The two most common, Lupus and Rheumatoid Arthritis, affect more than 2.3 million in the US alone, and result in at least 313,000 hospitalizations every year.
How to Contact others in our area.
http://www.marshallprotocol.com/forum3/353.html
MP Compliant Doctors in B.C.
Suggestions to get your Doctor on Board with the MP
http://www.marshallprotocol.com/forum2/238.html
It may help if you encourage your health care provider to join the
PRIVATE SECTION FOR MEDICAL PROFESSIONALS.
Please reassure him/her that many clinicians with little MP experience (including NPs and PAs) are helping their patients recover with the MP. S/he may ask questions in the private medical professionals only forum and let her/him know you can get 24/7 online support in managing the Herx reactions. These two resources (plus your own knowledge and compliance) should prevent any problems.
Your doctor may call Dr Marshall anytime to discuss treatment issues.
(805) 492-3693 or (805) 300-1679
Papers for Physicians, LINK
http://www.marshallprotocol.com/forum2/2274.html
Safety Warning to All
http://www.marshallprotocol.com/forum2/1071.html
Should I try to maintain a 'healthy alkaline' environment in my body?
http://www.marshallprotocol.com/forum32/7329.html
Dr. Greg Blaney
4419 West 10th Ave., Vancouver, BC, V6R 2H8
Ph: 604 224-6583 --- Fax: 604 224-6584
10/04 very enthusiastic and treating pts with the Marshall Protocol
Up-to-date Sarcoidosis Answers for Physicians, Nurses and Patients
Here at SarcInfo we have this disease BEATEN and on its knees.
Chronic Illness Support and Research Association (CISRA):
Synergy Health Newsletter
OTHER SOURCES:
-
American Academy of Environmental Medicine
- physicians who practice using alternative therapies. http://www.aaem.com/
Their address is 7701 E. Kellogg, Suite 625, Wichita, KS 67207 phone 316-684-5500.
-
The Australasian College of Nutritional and Environmental Medicine
has links to doctors all over the world including the USA: ACNEM Referrals
-
American College of Advancement in Medicine (ACAM)
- Send a self addressed, business size envelope with 55 cents postage to
American College. P. O. Box 3427, Laguna Hills, CA 92654
and ask for referral packet; call 1-800-532-3688 or visit their web site
http://www.acam.org/ where you can search for a doctor in your country and area.
ACAM doctors are often happy to prescribe antibiotics for RA.
- Physicians' names supplied by patients already on the MP.
You may find these by contacting any member of MP.com via private message or email.
-
The Arthritis Trust website - who also have a list of doctors.
http://www.arthritistrust.org/Physicians/ArthritisPhysicians.pdf
- Local pharmacists, your local health food store personnel or practitioners of any type of alternative medicine might be the source of information about doctors who are willing to consider the Marshall Protocol.
- Doctors who are just starting a practice are less likely to refuse patient requests for the Marshall Protocol.
- Nurse Practitioners and Physicians Assistants can also order the Marshall Protocol medications and supervise your treatment.
-
Contact MP.com members in your local area for information about their MP doctor.
�The Marshall Protocol for Treating Chronic Fatigue Syndrome:
Interview with Trevor Marshall, PhD,�
http://www.immunesupport.com/library/showarticle.cfm/id/5784
Following is an exclusive interview conducted in July 2004 with Trevor Marshall, PhD, who devised the highly demanding and still-controversial protocol, which must be administered under the care of a physician. He explains why he believes it may work for certain CFS and FM patients, and others. (See disclaimer at end of article.)
Question:
Please introduce yourself by giving some background on your medical training and practice.
Trevor Marshall, PhD:
I graduated Bachelor of Engineering (w/w statistics) from the University of Adelaide in 1974. I spent a year in Papua New Guinea teaching at the University of Technology in Lae, and then spent 6 years teaching at Curtin University in Western Australia. During that tenure I received my Masters Degree and commenced my PhD Research at the University of Western Australia, in Biomedical Engineering.
It was an exciting time.
Another UWA student, Dr. Barry Marshall (no relation) had just discovered that the bacterium Helicobacter Pylori was the cause of stomach ulcers, and the teaching hospital where we did our clinical research ("Sir Charles Gairdner") was full of "new ideas." My mentors were convinced that we needed to develop a totally different approach to medicine.
I researched Infertility and Cryptochidism with Ted Keough and Diabetes in Tim Welborn's group. Ted found a way to treat infertility by pulsatile infusion of a hormone called GnRH, and resolved Cryptorchidism without surgery, using pulsatile infusions of the hormone LHRH. Tim's group explored the continuous infusion of insulin in Diabetes.
After moving to the USA in 1982 I took some time off to study with Mike Albisser's group at the Hospital for Sick Children in Toronto. "Sick Kids" was a world leader in diabetes research at the time, and our research team included MDs and PhDs from all over the world. It was an amazing experience, and my doctoral thesis, "Mathematical Modeling of the Insulin Glucose Homeostasis in Healthy and Diabetic Individuals", was accepted in 1985.
... sunlight was a factor in immune disease, but it took many years for all the elements of the Th1 immune reaction to gel together in my mind. Late in 1999 I noticed that a new class of drugs, "Angiotensin Receptor Blockers' (ARBs), were affecting the psyche of Sarcoidosis patients. Since I knew that ARBs should not have any such effect I commenced a full-time sabbatical in early 2001 to try and figure out exactly what was happening.
The result ... a pathogenesis for sarcoidosis, published in 2002.
Since then we have conducted an Internet-based study of ARB and antibiotic therapy in sarcoidosis, and are now exploring how our success can be generalized to all the Th1 immune diseases.
The Autoimmunity Research Foundation is acting as a focus for our current efforts
(
http://autoimmunityresearch.org).
Question:
A number of patients with Chronic Fatigue Syndrome (CFS), Fibromyalgia (FM), and other chronic illnesses report they're finding success following your sarcoidosis treatment protocol. Could you explain what CFS, FM, and sarcoidosis patients might have in common that could explain this?
Trevor Marshall, PhD:
Sarcoidosis is a Th1 inflammatory disease which can damage the lungs, heart, eyes, brain, liver, kidneys and soul. Patients are still being told it has no known cause and no known cure.
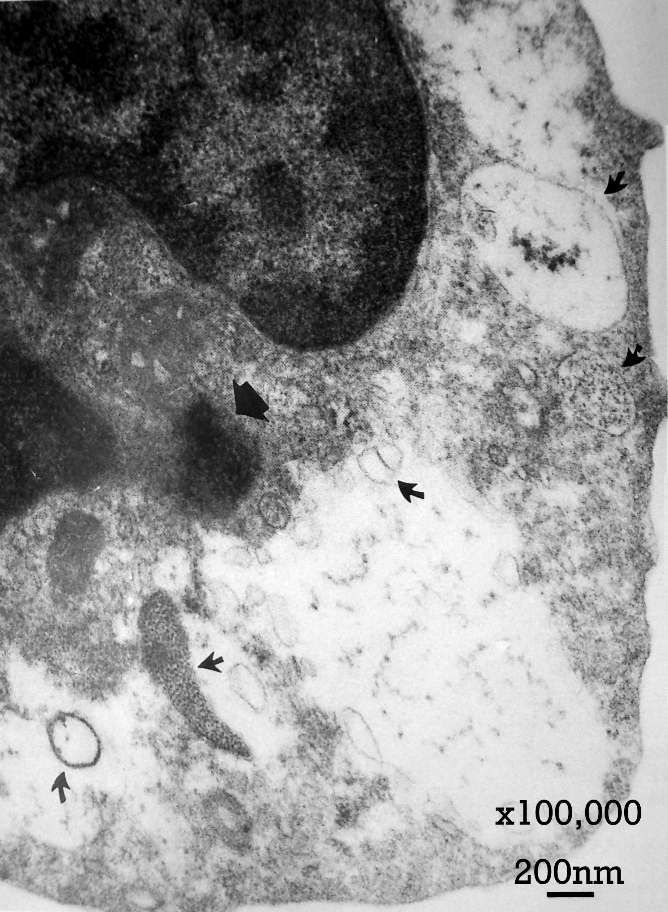
Tiny "pleomorphic" bacteria have been photographed living within the cells of the immune system of sarcoidosis patients. Emil and Barbara Wirostko produced stunning electron microscope photographs of immune phagocytes each containing hundreds of tiny bacterial forms, around 0.01 to 0.025 microns in diameter, living in colonies within the very cells (phagocytes) which are supposed to kill these bacterial parasites.
One of the Wirostko photographs can be found at
http://www.autoimmunityresearch.org/wirostko-fig3.jpg
It is important to understand that these bacteria are "coccoid" (round, and very, very small), 10 to 100 times smaller than the shapes these same pleomorphic bacteria will take when they enter the bloodstream.
We found that you can measure a hormone (in the blood) resulting from the Th1 inflammation produced by these tiny bacteria, and that it is elevated in Sarcoidosis patients. It is also often elevated in CFS patients, indicating that the inflammation of CFS is often very similar to that of Sarcoidosis.
Question:
Some researchers (including Garth Nicolson, PhD at The Institute for Molecular Medicine in Huntington Beach, California) and physicians believe that multiple co-infections including bacterial and mycoplasmal infections, play a key role in the onset and pathology of CFS and FM. To what extent are bacterial and mycoplasmal infections involved in sarcoidosis, and do you believe your methods for treating those infections in sarcoidosis apply to CFS and FM patients?
Trevor Marshall, PhD:
Multiple co-infections of antibiotic-resistant bacteria can act in unison because many of the species have evolved a similar technique for evading the immune system.
These bacteria live in the cytoplasm of phagocyte cells, and directly stimulate a protein called NuclearFactor-kappaB to cause the continuous release of inflammatory chemicals, a Th1 cytokine cascade. This is the source of the inflammation driving the CFS symptoms.
Where our work diverges from that of Dr. Nicolson is the manner in which we control the hormones Angiotensin II and 1,25-dihydroxyvitamin-D so as to weaken the defense mechanism of these tiny bacteria, and allow the immune system itself to start to recognize and kill them.
We then use common (oral) antibiotics, at a very low dosage, to help the immune system deal with the parasites. It is the immune system which kills these tiny resistant microbes, helped along by low-dose antibiotics.
Question:
... your treatment protocol for bacterial and mycoplasmal infections?
Trevor Marshall, PhD:
Our treatment protocol is split into two phases.
The first phase lasts for about three months and is focused on getting the bacterial load down to a point where the endotoxins are no longer life-threatening. Then, in phase 2, we use additional (low-dose) antibiotics, making it almost impossible for the resistant bacteria to evade the immune system.
Phase 1 is available online at
http://SarcInfo.com/phase1.pdf
We focus on blocking genetic protein transcription, the process whereby the tiny bacteria use the bacterial 30S and 50S Ribosomal Nucleic Acid subunits to produce the proteins they need to hide from the immune system.
In phase 2 we block multiple pathways for 50S RNA synthesis, which allows the immune system to recognize (and kill) even the strains which have evolved a resistance to standard antibiotics.
Question:
How do you go about improving immune function in your patients, what is your protocol for that objective which could cross over from sarcoidosis to CFS and FM patients?
Trevor Marshall, PhD:
The two hormones critical to this inflammatory process are Angiotensin II and the seco-steroid 1,25-dihydroxyvitamin-D.
Blockade of Angiotensin II weakens these bacteria to the point where they can be more easily killed, and reducing the 1,25-D makes it harder for the bacteria to slip in and out of the cells they have infected.
We use the Angiotensin Receptor Blocker "Olmesartan Medoxomil" (Benicar/Olmetec/Votum), dosed approximately every 6 hours, to blockade the Angiotensin II receptors in the inflamed tissue.
The seco-steroid 1,25-D is the active hormone resulting from sunlight on our skin, and the Vitamin D we ingest. Both these sources of 1,25-D have to be attenuated if these bacteria are to be killed.
Question:
Are you currently treating any patients with CFS and/or FM, or have you in the past?
If so, what is your strategy for treating these patients?
Trevor Marshall, PhD:
I am a researcher with a PhD, not an MD, and I cannot treat patients directly.
I help their physicians understand the disease process, so that those physicians can work with the patients to cure the disease. We are also working with several LLMDs (Lyme literate Medical Doctors).
I, and my colleagues, have published a number of papers describing all the elements of our discoveries, and, during 2002, we set up a clinical trial at the Internet site http://www.SarcInfo.com so that we could track the progress of the first patients using our protocol.
Also [a message board was created] called "MarshallProtocol" (http://www.marshallprotocol.com), and CFS and FM patients have used the information from that site to work with their physicians to implement the protocol... It seems the protocol is working just as well for these CFS and FM sufferers as it did for the sarcoidosis patients, most of whom have progressed to "cure" over the last two years.
Question:
... it is not unusual for someone with Lyme disease to be mis-diagnosed with CFS or FM. Could you discuss this issue, and talk a bit about how you diagnose and treat patients with Lyme and other spirochetal diseases?
Trevor Marshall, PhD:
Whether the inflammation (which gives rise to the CFS and/or FM symptoms) is caused by Borrelia, Bartonella, Chlamydia, or any other bacterium with the ability to change into these tiny pleomorphic shapes (also called "L-forms," "Cell Wall Deficient," "Cystic," "Mycoplasma"), the inflammation needs to be treated the same way. The microbes seem to be resistant to standard antibiotics, even IV antibiotics, and have to be killed by our immune system itself. We have defined what is necessary to achieve that.
Diagnosis can often be done from bloodwork assay.
If the level of 1,25-dihydroxyvitamin D in the blood is elevated (above 38-45pg/ml), or the 25-hydroxyvitamin-D depressed (below 20 ng/ml) then it is pretty certain that a Th1 process is in play (note: all blood must be frozen during transit to the labs for these tests to be accurate).
Sometimes it is quicker and cheaper to apply the angiotensin blockade as a "therapeutic probe." If there are profound psychic and systemic effects from using Benicar, a drug which usually only changes the blood pressure, then that is a pretty good indication of the presence of Th1 inflammation, and an indication it is worth starting on our protocol.
Question:
... specific laboratory tests to determine what infections they might have?
Trevor Marshall, PhD:
Unfortunately today's laboratory tests are of little use until the immune system starts to recognize these intracellular invaders. Hundreds of these tiny bacteria can live inside a single cell. They are too small to be seen with conventional optical microscopes. The host cells live for a relatively long time. There is little apoptosis (cell death), so very few bacteria are released into the bloodstream, and they are hard to detect with lab equipment.
Because they live in stable symbiosis with our immune system, there are no antibodies created. The bacteria live within the cells in stable colonies which cannot be attacked by the body's normal defenses. Lab tests will not find antibodies to these bacteria.
PCR (polymerase chain reaction testing) is capable of sensing the occasional cell apoptosis, but the resulting low DNA concentrations would be regarded as insignificant by most labs.
The biochemical symbiosis is so delicate that it is virtually impossible to culture these bacteria outside the body. Just as the bacteria causing Leprosy (mycobacterium leprae) and the bacteria causing Syphilis (treponema pallidum) are nearly impossible to culture, I expect it is unlikely we will be able to culture these Th1 pleomorphs until we fully understand the biochemistry needed to sustain them. No lab has been able culture these bacteria up to this point in time (with the possible exception of Lida Mattman's research at Wayne State University).
So I guess the next task for us is to start working with labs to help devise tests which can produce a reliable diagnosis.
Question:
Do you have any parting advice for CFS and FM patients seeking appropriate, effective treatment?
Trevor Marshall, PhD:
I would just say don't take "no" for an answer.
For the last 100 years sarcoidosis patients have been told that there is no known cause and no known cure for their disease (much the same prognosis being given to CFS and FM patients). The diagnosis of chronic sarcoidosis is regarded by pulmonologists as irreversible, they know their patient is dying, and that it is just a matter of time.
Yet the sarcoidosis folks who have been helping us develop our protocol, are becoming healthy again. Not just 10 percent, or 25 percent, but close to 100 percent are recovering their lives and their families.
They have variously reported regaining cognitive focus, stamina, and stable gait, and resolving chronic pain, paresthesias and visual disturbances. Some have been able to discard wheelchairs, braces and supplementary oxygen. ...
Benefit of testing for Rickettsia/The Marshal Protocol
I was diagnosed with Fibromyalgia/CFS some years ago. Then, after changing my doctor � who did many blood tests on my first visit � I was told that I actually have three strains of Rickettsia bacteria.
I am now being treated with antibiotics using �The Marshall Protocol�* [to rid the body of Rickettsia and similar tick, flea, and lice-borne bacteria-like organisms that colonize within the cells, too minute to be seen with an optical microscope] - which will kill off the parasite that is causing all of these problems, and hopefully I will go into good remission. Anyone who thinks they have FM or CFS should ask for a blood test for Rickettsia. This could be causing all the problems.
� Val
"
Recovery from Chronic Disease,"
http://autoimmunityresearch.org/chicago2005.htm
Our 2006 Conference in Los Angeles, had a focus on "Sarcoidosis, AutoImmunity, AIDS and Cancers."
The featured Guest Speaker was Dr Alan Cantwell, together with Honored Guest Prof. Yoshinobu Eishi.
The full 10 hours of Plenary and Panel sessions are contained on this DVD set, which has been factory-replicated for optimal compatibility with all DVD players and most computers.
the 2006 Los Angeles DVD set of Plenary Session, Panel sessions and Patient Tutorials, including Priority Mail within the USA: (Suggested donation $45:)
International: Please send me the 2 DVD set, International Priority Mail
(Suggested donation US$55)
DVD Pack for Physicians, Friends and Family
- "The Science" and "Recovery"
http://autoimmunityresearch.org/chicago2005.htm
This pack contains 4 DVDs - 2 each of "The Science," a compilation of Dr Marshall's recent presentations, and 2 each of "Recovering from Chronic Disease."
"The Science - Marshall Protocol."
This DVD contains the AAEM presentation, which runs for 1 hour 10 minutes (plus its Q&A session), explaining the science underpinning the MP. Additionally, Dr Marshall's presentation at Bio21, University of Melbourne, Australia, runs for 1 hour (plus Q&A), and his "Visiting Professor' presentation to the FDA runs for 55 minutes (plus Q&A ).
"Recovering from Chronic Disease"
Contains the 'Recovery' Panel Sessions from our 2005 and 2006 Conferences, and the 2006 Panel Session on 'Working with your Healthcare Provider' - altogether over a dozen patients describe what it is like to recover from Th1 diagnoses such as CFS, Rheumatoid Arthritis, Thyroiditis and Sarcoidosis.
US residents - please mail me the pack: (Suggested donation $20 to $40, as you can manage)
International: Please Airmail me the pack: (Suggested donation US $27 to $47)
Marshall Protocol Discussion Board
Before using the Board for the first time, please read the
"How to Register and Use this Board" forum
http://www.marshallprotocol.com/forum3/ located beneath the Topics of Discussion.
Please read the Board Policies
http://www.marshallprotocol.com/forum3/27.html
and instructions How to use the Board
http://www.marshallprotocol.com/forum3/36.html
If you have any questions, please post them in the General Discussion Forum.
The Board Policy is intended to keep the Board focused on productive discussion of the implementing of the Marshall Protocol. Please understand if we have to move, edit or delete some posts to achieve that goal. We will do our best to let you know if we have made modifications to any of your posts. We reserve the right to ban any member who repeatedly disregards Board Policies.
Unlike other boards, we do not provide emotional support.
Members may email or private message each other for extra support and encouragement.
You are cautioned about getting MP information/advice from other members off the Board as the advice may not be accurate.
Benefit of testing for Rickettsia/The Marshal Protocol
http://www.immunesupport.com/library/showarticle.cfm?id=7488&T=CFIDS_FM
I was diagnosed with Fibromyalgia/CFS some years ago.
Then, after changing my doctor � who did many blood tests on my first visit � I was told that I actually have three strains of Rickettsia bacteria. I am now being treated with antibiotics using �The Marshall Protocol�* [to rid the body of Rickettsia and similar tick, flea, and lice-borne bacteria-like organisms that colonize within the cells, too minute to be seen with an optical microscope] - which will kill off the parasite that is causing all of these problems, and hopefully I will go into good remission. Anyone who thinks they have FM or CFS should ask for a blood test for Rickettsia. This could be causing all the problems. � Val
MEMBERS on the Discussion Board and when joined, 04/2007.
Fri Jul 09th, 2004 --- Administration
Fri Jul 09th, 2004 --- Dr. Trevor Marshall, over 4,000 posts
Fri Jul 09th, 2004 --- Meg Mangin R.N., over 6,400 posts, Menomonie, Wisc
Sat Jul 10th, 2004 --- Belinda --------, almost 700 posts, Fort Worth, Texas
74 members in Texas, 55 in Washington, 39 in Illinois,
46 members in Michigan, 68 in Florida, 35 in North Carolina,
39 members in Ohio, 59 in Pennsylvania, 60 in New York,
Lesser numbers in most other states, no map numbers for outside USA.
We have 3955 members, 6988 topics, 94023 posts. (March 26, 2007)
Signature, max 255 characters
A Profile Signature is Required in order to Post
It will be added to the end of all Posts.
start dates and dose/schedule of Benicar - it is written as the necessarily precise 40 mg q6h (or q8h), rather than the imprecise 40 mg tid (three times a day) or 40 mg qid (four times a day).
-start dates and dose/schedule of minocycline
-NB: If you are in Phase two or three, do not include the name or dose of any Phase two or three antibiotic in your signature line, only the dates which you started phase two and three.
Examples:
Res/Pre MP?, Diagnosis, ALL Meds/supps I take, D tests April:1,25D=.. & 25D=.., avoiding light & D, NoIRs ordered/ Beni comm 11May Q6H, mino comm 6June: @..mg (< now dose), or phase 2 comm date..
Barb: Dx Inflammatory Disease Endocrine Imbalance 2003| 24+ years not Dx CFS| Cut D/exp July04| NoIR Aug04 Comm Beni|Q| Sept05 off Thyroxine| CLICK ABCofMP
Res MP, Dx ME-CFS from 2003; 3 wks on Doxycycline for Lyme in Mar, 2007; expect to follow with Pioglitazone (Actos) and Questran (cholestyramine); 9 Praziquantel to eliminate flukes-tapeworms Mar, 2007; considering Ozone, high dose B12, and IV supplements.
Link to high levels of Lead poisoning, 2008-02-22
This was confirmed by John R. Sennett as at least one significant factor contributing to this form of CFS-ME, benefited by the Marshall Protocol. Following the initial requirements of seclusion from daylight, wearing No-UV radiation wraparound sunglasses, and taking a daily combination of Benicar and
Minocycline. These measures, started in May, 2007, reduced his fatigued markedly within several months.
In late 2003, when John had acquired CFS-ME severe symptoms within days, he began to notice two peculiar symptoms. His skull appeared to expand such that his non tight fitting eyeglass frames gradually made an impression into the side of his head. He also frequently felt that his head was heavy or stuffy. He also noticed that while he had spent much of his life of 55 years out-of-doors and frequently found such to be invigorating, he was not now long out-of-doors before becoming severely fatigued. Planning any travel for business or pleasure became impossible. Over the next 4 years he would mention these symptoms to numerous doctors, medical specialists, alternative therapists .. only to receive blank stares.
During July, 2007, John took a 24-hr heavy metals challenge urine test.
In late August he received the results indicating a high presence of lead.
None had been indicated in a number of blood tests and hair analyses earlier and many intravenous chelation treatments had been taken over the previous 18 months. During October and November, John took TymBak water and Frequency Balancing treatments. By the end of December, John no longer tested positive to continue the Marshall Protocol and did not experience the rapid onset of fatigue when exposed to sunlight or products containing vitamin D.
John found the following references during his recovery.
-
Lead encephalopathy is a condition caused by extremely high levels of lead in the brain.
Lead causes the brain to swell, increasing pressure within the skull (cerebral edema), ...
Chelating agents for lead poisoning.
HealthWise Incorporated, 2007
http://members.kaiserpermanente.org/kpweb/healthency.do?
hwid=d52538231§ionId=d52538231-sec&contextId=hw119558
Lead encephalopathy is a condition caused by extremely high levels of lead in the brain. Lead causes the brain to swell, increasing pressure within the skull (cerebral edema), which can cause seizures, mental retardation, paralysis, blindness, coma, and death.
Canadian Centre for Occupational Health & Safety
http://www.ccohs.ca/oshanswers/chemicals/chem_profiles/lead/health_lead.html
EFFECTS ON THE CENTRAL NERVOUS SYSTEM:
Central nervous system (CNS) or brain function has been harmed in workers with long-term, low-level lead exposure. Symptoms typically occur with low to moderate exposure and include forgetfulness, irritability, tiredness, headache, fatigue, impotence, decreased libido (sexual drive), dizziness, and depression. ...
EFFECTS ON THE BLOOD AND HEART:
Inorganic lead can cause harmful effects to certain types of blood cells, including reduced hemoglobin production and reduced life span and function of red blood cells. Reduced hemoglobin production has been associated with low-level exposure to inorganic lead in the workplace. Hemoglobin is the molecule responsible for carrying oxygen to body tissues. ...
(encouraging Fatigue!, and, further assimilation of lead, in the absence of adequate iron.)
[ALL of these symptoms had been experienced, suddenly, and were reported.]
-
Impaired Vitamin D metabolism
[affecting bone remodelling, mineral absorption and calcium uptake]
http://www.lead.org.au/fs/fst7.html
Detailed in each of:
- "
Lead Poisoning Slide Show, 6 September 2000"
Dr. Ben Balzer, 32 slides, PowerPoint, 3. Meg
http://www.lead.org.au/bblp/bblp.html
-
Neurological perspective on lead toxicity.
Silbergeld, E. K. (1992).
In Human Lead Exposure,
ed H. L. Needleman, CRC Press.
-
Measuring lead exposure in infants children and other sensitive populations.
National Research Council (US). (1993).
National Academy Press, Washington DC.
- Low level health effects of lead:
Growth, developmental and neurological distrubances.
Schwartz, J. (1992).
In Human Lead Exposure,
ed H. L. Needleman, CRC Press
- Occupational and environmental lead exposure.
Fischbein, A. (1992).
In Environmental and Occupational Medicine, 2nd edn.
Ed W.N. Rom. Little, Brown & Co.
| {kind=link}
{kind=link}